Trigeminal Neuralgia Surgery
Trigeminal Neuralgia Surgery Video
In this video, Dr. Turner discusses trigeminal neuralgia surgery for both trigeminal neuralgia as well as atypical trigeminal neuralgia: discussing symptoms, success rate, and outcomes. He also discusses a different trigeminal neuralgia treatment as it relates to potentially fewer complications, lower risks, and from extensive experience, better recovery.
What is Surgery for Trigeminal Neuralgia?

We all know that there are many treatments & therapies for headaches and migraines. We also know that surgery has proven to be an invasive process that we firmly believe be carefully researched before deciding on. Such procedures may include gamma knife surgery or microvascular decompression surgery.
However, what if there was a natural way to fix these issues without surgery or procedures? Because now, our clinic has treated multiple thousands of patients from Texas and other countries with a unique treatment designed to stop & prevent the headaches and migraines at the source without surgery, injections, or medications!* The good news is that it tends to work for nearly all headache and/or migraine cases, often including other related symptoms and combination-type cases.*
To Learn More about what our clinic does, please see below.
Get Started With Texas Migraine Clinic or Learn More Below
*No upfront charges until you are approved, and consent to treatment.
*Please take the entire survey, or we cannot review your application.
*Still have Questions? CLICK HERE to visit our Quick-Answers FAQ HelpCenter.
How Does Surgery for Trigeminal Neuralgia Work?
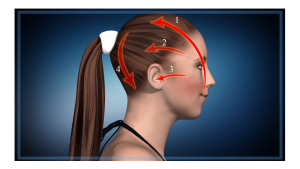
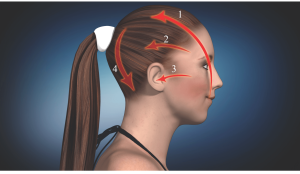
Migraine and headache specialist Dr. Turner here with Texas Migraine Clinic. You may have looked this up because of trigeminal neuralgia, and maybe you're looking for the best solution for that, just options and what our experience is. And I can tell you in 7,200 patients I've evaluated and treated over 18 years, I've seen lots of trigeminal neuralgia patients. And in fact, people that I see all day every day have trigeminal symptoms more frequently than any other symptom. And that is this trigeminal nerve, which you're probably familiar with if you're looking at this video.
The trigeminal nerve has three branches, one, two, three, hence the tri. And they cover the whole part of your head and face. And the difference between people who have the trigeminal symptoms, which is super common (like sinus issues, pressure, temple symptoms, ear pressure, tooth symptoms, jaw tightness) is that instead of it being spotty around here and just maybe intermittent then on both sides, commonly. With trigeminal neuralgia is typically on one side only, and it tends to go into the eye, cheek, jaw area, and cause all kind of mayhem with not constant symptoms, but more intermittent zappy kind of symptoms or sharp symptoms, very uncomfortable. And it can progress to where it's not just a moment in time. It's not just a little zap like if you brush your teeth, talk too much or whatever, or just doing nothing, zapping you, that it can get to where it can last even minutes at a time, just a large amount of pain.
So many go to desperate measures and often meds just aren't enough to manage it effectively. And people are looking for more than that. So, an option that we've seen over the years is microvascular decompressive surgery. And what that's about is making an incision behind your ear. Well, they shave your head back here, make an incision behind your ear, reflect the skin back and actually carve a hole in your skull. There's a suture there behind your neck and part of the sutures in your skull. And they carve a circle like that big around here at the base of your skull. So it's actually like a brain surgery. I mean, it is. And then the dura mater that covers your brains right under it. So they have to reflect that out of the way and split it apart with retractor thingys. I'm no expert on this. I'm just telling you what I've learned over the years.
And then deep to that, where they are at that certain location, they can view the trigeminal nerve, the branch of the trigeminal nerve. And their contention is that if we just take this blood vessel off, say it's an artery or a vein, and they can take that artery or vein and say, "this is the nerve, and this is artery or vein sitting on it". If they can put something in between those two, it's usually this piece of Teflon that separates them. It's like fuzzy Teflon, then they've decompressed it. That's the idea. And then once they are convinced that there's nothing compressing it all the way around circumferentially, then they put typically, best I could tell, I don't know if all of them do this, but they put this metal mesh thing on that's also a circle and they stick it to that area. And then they close you up and suture you up and that's that.
What to Expect After Trigeminal Neuralgia Surgery
So I admit it's very invasive. The effectiveness rate varies in the research from 80 to 94%, something like that. Pretty good outcomes for such a surgery, but very invasive. And there are always the risks of a surgery like that. And I mean, the list kind of goes on. You could look it up, which that's the first thing people tend to look at. Is what are the side effects of something like a brain surgery? But I mean, there could be infection, hearing loss, facial numbness, facial weakness, spinal fluid leak, difficulty with speech or swallowing. I mean, you get the idea. It's pretty invasive.
Well, our view after doing this for so many years, is that in our experience, not just our view, not our opinion, but actually real patients that we've relieved consistently of trigeminal neuralgia is that we found that the nerve, this trigeminal nerve branches, they're irritated, highly irritable, kind of like you cut your finger with a paper cut. Everybody's done that. And you know how sensitive it is, super sensitive. And then next thing you know, you can do this say four days later and you don't really feel anything except you touching herself, but it's not that zappy pain.
Well, that's how the trigeminal nerve behaves in our experience that this area down in here in the mid to lower neck, there are lots of structures here that feed right up the spinal cord, this pink thing right here, this is the brainstem that turns into the spinal cord, feeds this nerve irritation right at the spinal cord. That's what the purple dash line is, is nerve irritation. And that's how it flows right into CNC, goes right into that nerve system. And what we do is we shut it off from down here, we fix the problems in here. It's a hyper specialty to do that, but that's what we do, is fix these kinds of problems to calm that nerve system down. So in our view, it doesn't need to be decompressed. And it's not just our view. I mean, when the symptoms go to zero consistently, you obviously don't need to have a procedure done.
So we think the nerve is just upregulated and irritable, or that's the best explanation of why we can fix these problems out here and stop that nerve irritation from going into those nerve systems. So I just discharged a patient about, it's been two and a half weeks ago, with trigeminal neuralgia, horrible, and she didn't need to have surgery. She doesn't need to take medications now. And it's cleared. That's just an example.
And we did a study, an MD colleague and I, who'd seen many patients together over seven years. But we had one study where we just saw 10 consecutive trigeminal neuralgia patients to gather data on and we didn't drop any of them. They're all just consecutive patients in the study. And we presented this at a symposium, like a headache, migraine symposium, and all 10 of them got to zero consistently, no medication, no surgery and official diagnosis of trigeminal neuralgia. As an example, that's the difference between the two. And it always seemed to make sense to me to go conservative before not conservative, considering how conservative this system is with no surgery, no meds, no injections or anything like that. And in the end, generally no ongoing meds either.
But if this sounds like it's something interesting to you and you think you might be a fit, but you're not sure, you can go to our website and just fill out the survey and just submit it. And then somebody from our office will contact you. Take care, and thanks.
How To Find if We're a Good Fit for a Particular Headache or Migraine Case
After evaluating and treating many clients, we have accurate data to determine with high accuracy whether or not treatment applicants are a good fit before treatment before they decide to have it.
Being from another country other than Texas isn't necessary because of the highly developed NerveCode™ remote treatment program we use for clients outside of Texas. We've found the relief results of the NerveCode™ remote program to be just as effective as the in-clinic cases we've seen in Texas.
To learn if a particular case is a good fit, feel free to take the survey below.
*No upfront charges until you are approved, and consent to treatment.
*Please take the entire survey, or we cannot review your application.
*Still have Questions? CLICK HERE to visit our Quick-Answers FAQ HelpCenter.
Q&A: Answers
Trigeminal neuralgia causes, and what causes trigeminal neuralgia to flare up?
We've found these issues to be correlated to up-regulation of, mainly, obstruction of the trigeminal nerve. These issues are regularly sorted out with the custom Treatment we use.
What is the latest and new treatment for trigeminal neuralgia?
The Advanced Treatment we've been using has been around for quite some time, being highly developed at this point. However, we believe that there's an answer in most cases to these symptoms & causes without the need for invasive trigeminal neuralgia surgery.